
To Bind Up the Nation's Wounds
Trauma and Surgery
"The Smell of Ether, the Odor of Blood"
 Popular but generally incorrect images of Civil War medicine involve surgery-amputations without anesthesia, piles of arms and legs, the surgeon as a butcher. By modern standards, wartime surgery was limited. Despite the lack of both surgical experience and sanitary conditions, the survival rate among those who underwent the knife was better than in previous wars. Amputation was not the only surgical recourse available. Surgeons also extracted bullets, operated on fractured skulls, reconstructed damaged facial structures, and removed sections of broken bones.
Popular but generally incorrect images of Civil War medicine involve surgery-amputations without anesthesia, piles of arms and legs, the surgeon as a butcher. By modern standards, wartime surgery was limited. Despite the lack of both surgical experience and sanitary conditions, the survival rate among those who underwent the knife was better than in previous wars. Amputation was not the only surgical recourse available. Surgeons also extracted bullets, operated on fractured skulls, reconstructed damaged facial structures, and removed sections of broken bones.
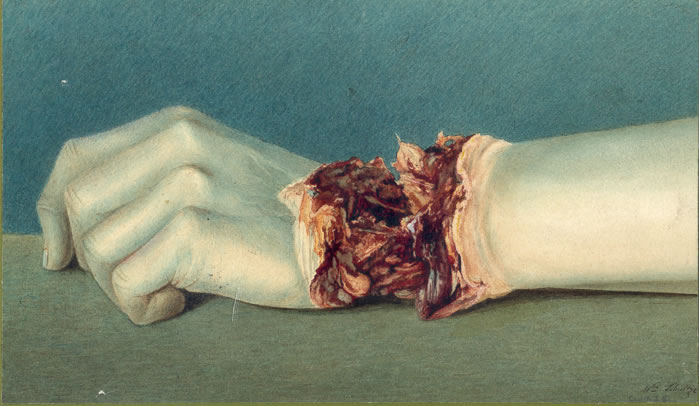 As bullets hit their victims, shattered bone and shredded flesh became the calling cards of the minie ball. Most of the surgeons who had come from civilian practices had little or no experience in dealing with such wounds. They quickly became aware of the surgical options: remove the limb, remove the fractured portions of bone, or clean the wound and apply a dressing. Union surgeons documented nearly 250,000 wounds from bullets, shrapnel, and other missiles. Fewer than 1,000 cases of wounds from sabers and bayonets were reported.
As bullets hit their victims, shattered bone and shredded flesh became the calling cards of the minie ball. Most of the surgeons who had come from civilian practices had little or no experience in dealing with such wounds. They quickly became aware of the surgical options: remove the limb, remove the fractured portions of bone, or clean the wound and apply a dressing. Union surgeons documented nearly 250,000 wounds from bullets, shrapnel, and other missiles. Fewer than 1,000 cases of wounds from sabers and bayonets were reported.
The Case of Major General Daniel E. Sickles
 Major General Daniel E. Sickles, Union Third Army Corps commander, was struck by a cannonball during the battle of Gettysburg. Sickles was on horseback when the 12-pound ball severely fractured his lower right leg. Sickles quieted his horse, dismounted, and was taken to a shelter where Surgeon Thomas Sims amputated the leg just above the knee. Shortly after the operation, the Army Medical Museum received Sickles' leg in a small box bearing a visiting card with the message "With the compliments of Major General D.E.S." The amputation healed rapidly and by September of 1863 Sickles returned to military service. For many years on the anniversary of the amputation, Sickles visited his leg at the museum.
Major General Daniel E. Sickles, Union Third Army Corps commander, was struck by a cannonball during the battle of Gettysburg. Sickles was on horseback when the 12-pound ball severely fractured his lower right leg. Sickles quieted his horse, dismounted, and was taken to a shelter where Surgeon Thomas Sims amputated the leg just above the knee. Shortly after the operation, the Army Medical Museum received Sickles' leg in a small box bearing a visiting card with the message "With the compliments of Major General D.E.S." The amputation healed rapidly and by September of 1863 Sickles returned to military service. For many years on the anniversary of the amputation, Sickles visited his leg at the museum.
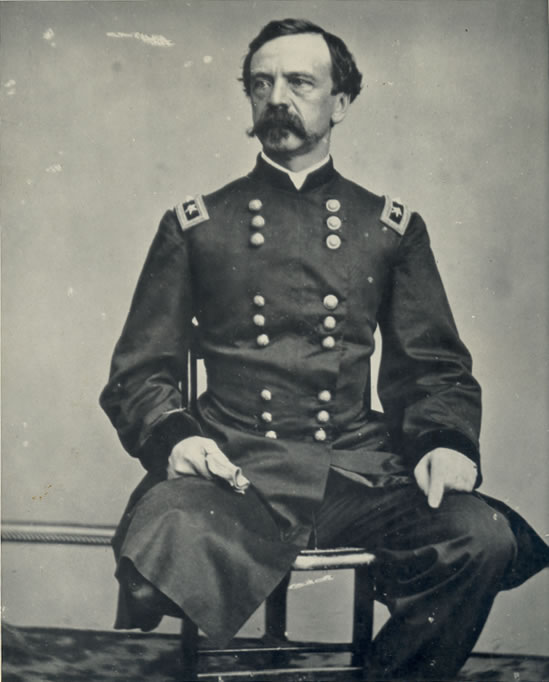 Sickles' exploits extended beyond the Civil War. He was the first defendant to successfully use the temporary insanity defense in the United States. In 1859, Sickles was found not guilty of the murder of his wife's lover, Philip Barton Key, the son of the composer of the national anthem. Sickles had shot Key in Lafayette Square in Washington in a jealous rage after learning of the affair. Sickles served as a secret agent for President Lincoln and was appointed Ambassador to Spain by President Grant.
Sickles' exploits extended beyond the Civil War. He was the first defendant to successfully use the temporary insanity defense in the United States. In 1859, Sickles was found not guilty of the murder of his wife's lover, Philip Barton Key, the son of the composer of the national anthem. Sickles had shot Key in Lafayette Square in Washington in a jealous rage after learning of the affair. Sickles served as a secret agent for President Lincoln and was appointed Ambassador to Spain by President Grant.
Anesthesia
 Anesthesia was an important surgical advance introduced a few decades before the Civil War. Ether or chloroform was applied to a cloth cone that was placed over the mouth and nose of the patient. The patient became stuporous in a matter of minutes. This state lasted for more than enough time to perform an amputation, which took about 6 minutes to complete. Union surgeons used anesthesia in more than 80,000 operations.
Anesthesia was an important surgical advance introduced a few decades before the Civil War. Ether or chloroform was applied to a cloth cone that was placed over the mouth and nose of the patient. The patient became stuporous in a matter of minutes. This state lasted for more than enough time to perform an amputation, which took about 6 minutes to complete. Union surgeons used anesthesia in more than 80,000 operations.
Since anesthesia was available, Civil War surgeons attempted new operative procedures to contend with some of the severe wounds they encountered. One such procedure, reconstructive surgery of the face, involved suturing together the soft tissues of the eyelids, nose, and mouth. Sometimes extensive rebuilding of the underlying bone with splints and surgical fixtures was required. Surgeons performed more than 30 of these operations.
The Case of Private Carleton Burgan
Private Carleton Burgan, B Company, Purnell's Maryland Legion, age 20, was admitted to the general hospital in Frederick, Md., on Aug. 4, 1862, with pneumonia. He was given calomel, a strong mercurial drug. On Aug. 6, doctors discovered that the calomel had caused an ulcer on Burgan's tongue. The ulcer soon spread to his cheek and the roof of his mouth. The ulcer became gangrenous. The gangrene disappeared on Aug. 27, but it had destroyed Burgan's upper mouth, palate, right cheek and right eye. The bone of his right cheek was removed to halt any further spread of the gangrene.
Burgan's condition made him a candidate for reconstructive surgery. Dr. Gurdon Buck of City Hospital in New York performed a series of operations to rebuild Burgan's face. Dental and facial fixtures were crafted to fill in the missing bone and support the skin. Burgan's case was the first involving total facial reconstructive surgery. He went on to live a normal life, with minimal visual and physical reminders of the damage.

|

|

|

|
|
Engravings showing Burgan at various stages during his surgery.
|
|||
Infection
 Although fortunate to be unconscious during surgery, soldiers who underwent the knife often received a nasty visitor a few days later-infection. Any open wound almost always became infected. The unwashed hands of the surgeon, the non-sterile surgical instruments used on a succession of men, and the dirty sponges used on an entire ward of wounded soldiers all introduced infectious bacteria into wounds. These infections often resulted in gangrene and death.
Although fortunate to be unconscious during surgery, soldiers who underwent the knife often received a nasty visitor a few days later-infection. Any open wound almost always became infected. The unwashed hands of the surgeon, the non-sterile surgical instruments used on a succession of men, and the dirty sponges used on an entire ward of wounded soldiers all introduced infectious bacteria into wounds. These infections often resulted in gangrene and death.
Case of Private Julius Fabry
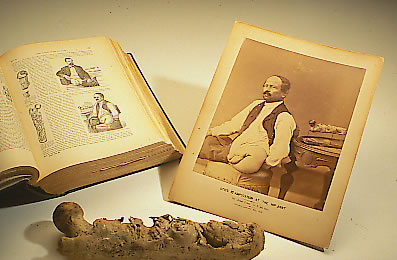
Private Julius Fabry, K Company, 4th U.S. Artillery, age 38, was shot in the left knee at the battle of Deep Bottom, Virginia, on Aug.16, 1864. His leg was amputated just above the knee on the following day. The thigh bone became infected and Fabry's pain was treated with morphine for the next 6 years. Pus drained regularly from the infected bone. In 1870, the infected bone was remove at the hip joint. In 1878, Fabry reported no trouble with the stump, but he was unwilling to use an artificial limb. Fabry died in 1894.Amputation
 Surgeons frequently treated arm and leg wounds by amputating. The grisly wounds caused by bullets and schrapnel were often contaminated by clothing and other debris. Cleaning such a wound was time-consuming and often ineffective. However, amputation made a complex wound simple. Surgical manuals taught that an amputation should be performed within the first two days following injury. The death rate from these so-called primary amputations was lower than the rate for amputations performed after the wound became infected. Union surgeons performed nearly 30,000 amputations.
Surgeons frequently treated arm and leg wounds by amputating. The grisly wounds caused by bullets and schrapnel were often contaminated by clothing and other debris. Cleaning such a wound was time-consuming and often ineffective. However, amputation made a complex wound simple. Surgical manuals taught that an amputation should be performed within the first two days following injury. The death rate from these so-called primary amputations was lower than the rate for amputations performed after the wound became infected. Union surgeons performed nearly 30,000 amputations.
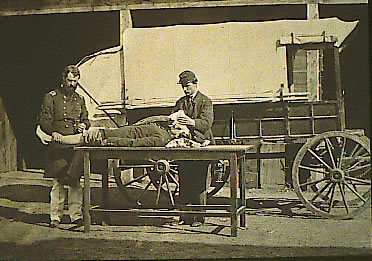
 Patients undergoing amputation were first anesthetized. A tourniquet was applied above the site of the proposed amputation. The skin and muscle were then cut with amputation knives several inches above the fracture site. The muscles were pulled up to expose the bone. An amputation saw was used to cut through the bone. Once the cut was completed, large arteries were pulled out from the stump tissue with a tenaculum and tied off to prevent bleeding. The skin muscle was then released and the tissue sutured. Two types of amputation were commonly used. A circular amputation involved cutting straight through the skin to the bone and resulted in a stump that was circular in appearance. A flap amputation required the tissue to be cut leaving two flaps of skin that were used to create a stump. Fingers and other small bones were amputated using the smaller metacarpal saw.
Patients undergoing amputation were first anesthetized. A tourniquet was applied above the site of the proposed amputation. The skin and muscle were then cut with amputation knives several inches above the fracture site. The muscles were pulled up to expose the bone. An amputation saw was used to cut through the bone. Once the cut was completed, large arteries were pulled out from the stump tissue with a tenaculum and tied off to prevent bleeding. The skin muscle was then released and the tissue sutured. Two types of amputation were commonly used. A circular amputation involved cutting straight through the skin to the bone and resulted in a stump that was circular in appearance. A flap amputation required the tissue to be cut leaving two flaps of skin that were used to create a stump. Fingers and other small bones were amputated using the smaller metacarpal saw.
Prosthetic limbs were designed and built to help amputees regain some of their former capabilities. Some of these devices were custom-made while others were mass-produced.
The Case of Private Columbus Rush
Private Columbus Rush, Company C, 21st Georgia, age 22, was wounded during the assault on Fort Stedman, Virginia, on March 25, 1865 by a shell fragment that fractured both the right leg below the knee and the left kneecap. Both limbs were amputated above the knees on the same day. He recovered quickly and was discharged from Lincoln Hospital in Washington on Aug. 2, 1865. In 1866, while being treated at St. Luke's Hospital in New York City, he was outfitted with artificial limbs.

|

|
|
The results of the double amputation.
|
Using his prosthetic legs, Rush could
walk with the aid of two canes. |
Excision
 Surgeons treated some shoulder wounds with a technique known as excision, also termed exsection or resection.
Surgeons treated some shoulder wounds with a technique known as excision, also termed exsection or resection.  The fractured bone was removed, the tissues sutured, and the limb left to heal. Excision gave the patient limited use of the arm and usually full use of the hand. Prosthetic braces worn over the shoulder allowed nearly normal function of the limb for some patients.
The fractured bone was removed, the tissues sutured, and the limb left to heal. Excision gave the patient limited use of the arm and usually full use of the hand. Prosthetic braces worn over the shoulder allowed nearly normal function of the limb for some patients.
The Case of Private J.P. Kegerreis
Private J.P. Kegerreis, Company B, 2nd Pennsylvania Heavy Artillery, was wounded at Petersburg, Va. on June 17, 1864 by a minie ball. The ball entered his neck, punctured his windpipe, and passed through his right shoulder joint and out his back. Keggereis was tagged for amputation at the field hospital but tore off the tag and crawled among the less seriously wounded. Three days later, while at City Point Hospital, his wound was treated and found filled with maggots. His neck wound healed in a month, but his shoulder wound was infected. In the winter of 1865, the infected bone was removed by excision. The wound healed slowly, and he was discharged in May of 1866. In December of 1867, a surgeon removed a large piece of bone from the joint and the bones of the arm later fused on a semi-flexed position. He was able to lift 135 pounds with his injured arm.Conservation
 Conservative treatment was employed in the cases of flesh wounds or minor bone fractures. The wound was cleaned of bone fragments, clothing, and other debris and dressed with bandages. Local anesthetic was often applied. Conservation left the limb intact, but the use of unsterilized instruments, unwashed hands, and dirty bandages often introduced infection.
Conservative treatment was employed in the cases of flesh wounds or minor bone fractures. The wound was cleaned of bone fragments, clothing, and other debris and dressed with bandages. Local anesthetic was often applied. Conservation left the limb intact, but the use of unsterilized instruments, unwashed hands, and dirty bandages often introduced infection.
The Case of Corporal G.W. Stone
Corporal G.W. Stone, Company A, 12th Massachusetts was wounded at Fredericksburg, Va. on Dec. 13, 1862, when a conoidal ball penetrated his right eye and lodged behind his left eye. His only exterior symptoms were a small wound to the lid of his right eye and the slight protuberance of his left eye. His left eye continued to function normally. Corporal Stone complained only of a slight headache. The wound to his right eye healed well, and within in three weeks, he was allowed to walk about the city with a hospital pass. Suddenly on Feb. 6, 1863, he developed chills. Fever and delirium followed. He died at midnight on Feb. 15, 1863.
The Case of Private John Tucker
 Private John Tucker, 17th Maine, age 20, was wounded by a shell explosion at the battle of Chancellorsville, Va. on May 3, 1863. The shell removed a large portion of the skin and muscle of the buttocks and lower back. Applications of wet lint doused with disinfectant lotion were used to treat the wound. Several days later he contracted tetanus and was treated with olive oil applied to cotton batting and with doses of morphine. He survived the tetanus. By 1870, part of the wound remained an open ulcer that drained a thick pus. The doctor recommended the new technique of skin grafting to heal the wound but it is unknown if Tucker underwent the operation.
Private John Tucker, 17th Maine, age 20, was wounded by a shell explosion at the battle of Chancellorsville, Va. on May 3, 1863. The shell removed a large portion of the skin and muscle of the buttocks and lower back. Applications of wet lint doused with disinfectant lotion were used to treat the wound. Several days later he contracted tetanus and was treated with olive oil applied to cotton batting and with doses of morphine. He survived the tetanus. By 1870, part of the wound remained an open ulcer that drained a thick pus. The doctor recommended the new technique of skin grafting to heal the wound but it is unknown if Tucker underwent the operation.
Head Wounds
 Head wounds were not always fatal. A soldier's prognosis was best when bone splinters were removed and the wound was left to heal. In more severe wounds, trephination was used. Trephination involved drilling a circular hole into the skull to relieve pressure from bleeding or to remove fragments of bone pressing on the brain. Trephinations were fatal in over half of the 220 operations performed by Union surgeons.
Head wounds were not always fatal. A soldier's prognosis was best when bone splinters were removed and the wound was left to heal. In more severe wounds, trephination was used. Trephination involved drilling a circular hole into the skull to relieve pressure from bleeding or to remove fragments of bone pressing on the brain. Trephinations were fatal in over half of the 220 operations performed by Union surgeons.
 To perform a trephination, the patient was first anesthetized. The tissue surrounding the trephination site was then pulled back and the trephine placed on the site. The trephine was turned in a circular motion to slowly cut through the bone. Care was taken not to cut the tissue surrounding the brain. An instrument called an elevator was used to raise sections of fractured bone away from the brain. A Heye's saw was used to remove protruding bone fragments.
To perform a trephination, the patient was first anesthetized. The tissue surrounding the trephination site was then pulled back and the trephine placed on the site. The trephine was turned in a circular motion to slowly cut through the bone. Care was taken not to cut the tissue surrounding the brain. An instrument called an elevator was used to raise sections of fractured bone away from the brain. A Heye's saw was used to remove protruding bone fragments.
The Case of Private J. Luman
Private J. Luman of Company A, 122nd Ohio Volunteers was wounded at the battle of Mine Run, Va. on Nov. 27, 1863, when a minie ball passed through his skull. He was treated in the field hospital for several days before being evacuated to the 3rd division hospital in Alexandria. By Dec. 8, Private Luman was comatose, and Surgeon E. Bentley applied a trephine and removed the splinters of bones associated with the wound. His condition failed to improve and he died five days later.
The Case of Corporal G.H. Swift
Corporal G.H. Swift, Company C, 18th Massachusetts, was injured at the battle of Chancellorsville, Va. on May 3, 1863, when a musket ball fractured the top of his skull. Surgeons attempted to trephine the wound but halted the procedure upon discovering that the inner surface of the skull was not fractured. Corporal Swift died on May 17.Chest and Abdominal Wounds
 Chest and abdominal wounds were nearly always fatal. Treatment of abdominal wounds often involved pushing in protruding organs and suturing the wound. Food was withheld because fecal material leaking from the intestines caused contamination. Opium was often administered to halt the action of the digestive system. Abdominal wounds were fatal in almost 90 percent of the cases reported by Union surgeons. Chest wounds were cleaned and the wound was sutured.
Chest and abdominal wounds were nearly always fatal. Treatment of abdominal wounds often involved pushing in protruding organs and suturing the wound. Food was withheld because fecal material leaking from the intestines caused contamination. Opium was often administered to halt the action of the digestive system. Abdominal wounds were fatal in almost 90 percent of the cases reported by Union surgeons. Chest wounds were cleaned and the wound was sutured.
The Case of Major General Henry Barnum
 Major General Henry A. Barnum of the 12th New York was injured at Malvern Hill, Va. on July 1, 1862, by a musket ball that passed through his left lower abdomen. The ball penetrated his intestines and hip bone. The wound was considered fatal and he was left in a field hospital. A few days later he was captured and taken 18 miles to Libby Prison. Fifteen days later he was transported 17 miles and exchanged. In October, the wound was opened and several bone fragments were removed. He was promoted to Colonel in January of 1863 and sent back to the field. A year later, Barnum visited a private physician who pushed a probe through the wound causing a large abscess to drain. In order to keep the wound draining, the physician threaded a probe with a strip of oakum and passed it through the wound. Barnum wore a thread through the wound his entire life. He was promoted to Brigadier General and was also injured in battles at Kenesaw Mountain and Peachtree Creek, Ga.. Barnum died of pneumonia at the age of 65 still wearing a thread through the wound.
Major General Henry A. Barnum of the 12th New York was injured at Malvern Hill, Va. on July 1, 1862, by a musket ball that passed through his left lower abdomen. The ball penetrated his intestines and hip bone. The wound was considered fatal and he was left in a field hospital. A few days later he was captured and taken 18 miles to Libby Prison. Fifteen days later he was transported 17 miles and exchanged. In October, the wound was opened and several bone fragments were removed. He was promoted to Colonel in January of 1863 and sent back to the field. A year later, Barnum visited a private physician who pushed a probe through the wound causing a large abscess to drain. In order to keep the wound draining, the physician threaded a probe with a strip of oakum and passed it through the wound. Barnum wore a thread through the wound his entire life. He was promoted to Brigadier General and was also injured in battles at Kenesaw Mountain and Peachtree Creek, Ga.. Barnum died of pneumonia at the age of 65 still wearing a thread through the wound.