
To Bind Up the Nation's Wounds
Evacuation and Hospitalization
"Some on the Bare Ground, Some on Planks and Stretchers"
The first battles revealed gaping holes in the capabilities of the medical commands to evacuate wounded men from the battlefield, render immediate care, and arrange long-term hospitalization. Outdated military regulations relied on regimental musicians to remove the wounded. Surgeons were required to treat only men from their assigned regiment, but even then they were soon overwhelmed by the chaos of battle. In some cases, days passed before men were removed from the battlefields. Townspeople became nurses. Their carts and wagons served as ambulances and their homes were outfitted into makeshift hospitals.
The public and military medical personnel grew outraged by these conditions. Their reactions forced significant changes in evacuation and hospital systems. Troops were organized and trained to recover and transport wounded men in ambulances. New types of ambulances were designed and built. Railcars and ships were outfitted to move the wounded from field hospitals to general hospitals. Large general hospitals holding thousands of patients and hospitals specializing in particular diseases and medical conditions were built. Surgeons planned the location of evacuation points and field hospitals before battles commenced. The procedures developed during the Civil War-rapid evacuation, assessment in the field, and transportation to a hospital far from the battle lines-are still in use by the American military.

The Rucker ambulance could carry men
in both the sitting and lying position. (CP 1513) |

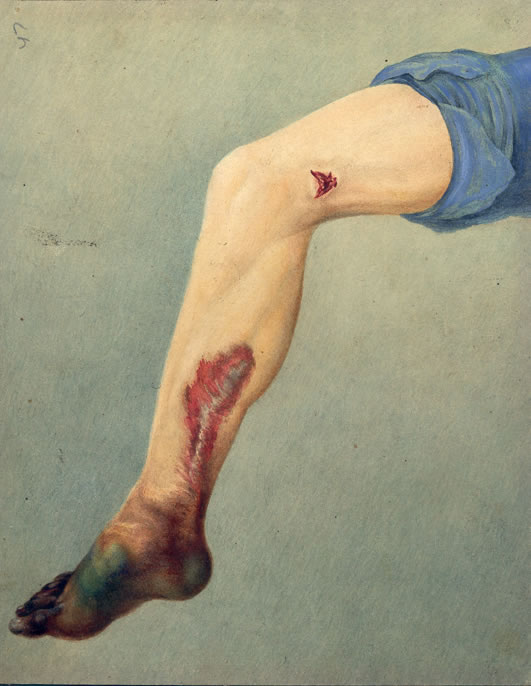
Private Milton E. Wallen, C Company, 1st Kentucky Cavalry was being treated for gangrene in August 1863 when Edward Stauch traveled from Washington to make this sketch. Wallen survived the infection and was furloughed from the hospital in October 1863.
|
Hospitalization
Once evacuated from the battlefield, wounded soldiers were evaluated at the field hospital. Three categories were used- the walking wounded, the wounded requiring immediate care, and the wounded beyond help. The walking wounded were given opium for pain and their wounds were cleaned and dressed. Immediate care usually involved amputation or bullet extraction. Morphine and opium were given to the fatally wounded. Once treated, the wounded were then evacuated to larger division and general hospitals.
 Field hospitals were established in tents, barns, houses, or other protected locations with access to water. Hastily erected rows of tents also served this purpose. The usual means of evacuation to a field hospital were stretchers, two-wheeled ambulances, or on the shoulder of a fellow soldier.
Field hospitals were established in tents, barns, houses, or other protected locations with access to water. Hastily erected rows of tents also served this purpose. The usual means of evacuation to a field hospital were stretchers, two-wheeled ambulances, or on the shoulder of a fellow soldier.
With the influx of large numbers of sick and wounded soldiers, the cities of the eastern and southern coasts became centers for large general hospitals. New hospitals were designed and built. Others were created from existing buildings. A belief that "bad air" caused certain diseases suggested that increased airflow would reduce sickness. As a result, new hospitals maximized the ventilation of the wards.
 Some hospitals specialized in the care of certain injuries or medical conditions. For example, Turner's Lane Hospital in Philadelphia became the Union Army's hospital for the care of neurological disorders. The Confederate medical command favored the construction of very large hospitals. With 8,000 beds and 250 surgeons, Chimborazo Hospital in Richmond was one of the largest.
Some hospitals specialized in the care of certain injuries or medical conditions. For example, Turner's Lane Hospital in Philadelphia became the Union Army's hospital for the care of neurological disorders. The Confederate medical command favored the construction of very large hospitals. With 8,000 beds and 250 surgeons, Chimborazo Hospital in Richmond was one of the largest.
 The sanitary conditions in some wards often led to "hospital gangrene." Sergeant G.W. Gardner, age 29, Company A, 12th Illinois Cavalry, was shot through the leg with a conoidal carbine ball at Mitchell's Ford, Va., on Oct. 11, 1863. The ball, which did not strike bone, was removed, and Gardner was sent by train to Emory Hospital in Washington. Following treatments of hot water, oxygen gas, and cotton packing, gangrene of the foot set in and spread rapidly up the leg. The leg was amputated on Oct. 29. Gardner contracted diarrhea soon after the amputation and died on Dec. 5, 1863.
The sanitary conditions in some wards often led to "hospital gangrene." Sergeant G.W. Gardner, age 29, Company A, 12th Illinois Cavalry, was shot through the leg with a conoidal carbine ball at Mitchell's Ford, Va., on Oct. 11, 1863. The ball, which did not strike bone, was removed, and Gardner was sent by train to Emory Hospital in Washington. Following treatments of hot water, oxygen gas, and cotton packing, gangrene of the foot set in and spread rapidly up the leg. The leg was amputated on Oct. 29. Gardner contracted diarrhea soon after the amputation and died on Dec. 5, 1863.
Harewood Hospital
As the war progressed, Washington became home to several hospitals. Some were new constructions while others were in renovated buildings. Harewood Hospital was located on 7th Street, NW, near the Soldiers Home. Harewood was supervised by Surgeon Reed Bontecou. It held 2,000 beds in the permanent wards. At one time 312 hospital tents holding 1,872 beds were also on the grounds.
Transportation of the Wounded
 Two military physicians were largely responsible for the changes in evacuation procedures and the system of hospital care during the war. Union surgeon Jonathan Letterman, medical director for the Army of the Potomac, was instrumental in establishing regimental aid stations, field hospitals, and division level hospitals. He also authorized training for ambulance companies responsible for moving wounded men from the battlefield to the field hospital. Dr. Samuel Stout, of the Confederate medical service, established aid stations, devised mobile field and general hospitals (the origins of the MASH unit), and championed hospitals with large, open wards. He also organized effective evacuation systems for wounded Confederates. The changes instituted by Stout and Letterman-rapid evacuation, assessment in the field, and transportation to a hospital far from the battle lines-provided sick and wounded soldiers a process of care still used by the American military.
Two military physicians were largely responsible for the changes in evacuation procedures and the system of hospital care during the war. Union surgeon Jonathan Letterman, medical director for the Army of the Potomac, was instrumental in establishing regimental aid stations, field hospitals, and division level hospitals. He also authorized training for ambulance companies responsible for moving wounded men from the battlefield to the field hospital. Dr. Samuel Stout, of the Confederate medical service, established aid stations, devised mobile field and general hospitals (the origins of the MASH unit), and championed hospitals with large, open wards. He also organized effective evacuation systems for wounded Confederates. The changes instituted by Stout and Letterman-rapid evacuation, assessment in the field, and transportation to a hospital far from the battle lines-provided sick and wounded soldiers a process of care still used by the American military.
 Once evaluated and cared for at the field hospital, wounded men were transported to general hospitals in trains and hospital ships. Large numbers of wounded men could be loaded on these trains and ships, given care, and transported directly to general hospitals. Hospital trains could carry hundreds of patients. Many contained kitchens and well-spaced bunks to provide better patient care. Ships transported soldiers to general hospitals and also served as floating hospitals. Later in the war, Union ships stopped at Southern ports to pick up wounded and transport them up the Atlantic coast to hospitals in Washington, Philadelphia, and New York.
Once evaluated and cared for at the field hospital, wounded men were transported to general hospitals in trains and hospital ships. Large numbers of wounded men could be loaded on these trains and ships, given care, and transported directly to general hospitals. Hospital trains could carry hundreds of patients. Many contained kitchens and well-spaced bunks to provide better patient care. Ships transported soldiers to general hospitals and also served as floating hospitals. Later in the war, Union ships stopped at Southern ports to pick up wounded and transport them up the Atlantic coast to hospitals in Washington, Philadelphia, and New York.
 The U.S. Army Hospital Steamer DA January was a side-wheel steamer that served as a floating hospital. Outfitted to allow for the best in patient care, it contained a surgical suite, baths, a kitchen, nurses quarters, hot and cold running water, and an ice water cooler. Windows circulated air through the wards, which held nearly 450 beds. During its four years of service, the DA January transported and cared for more than 23,000 wounded men. It regularly visited the cities along the Mississippi and Ohio rivers.
The U.S. Army Hospital Steamer DA January was a side-wheel steamer that served as a floating hospital. Outfitted to allow for the best in patient care, it contained a surgical suite, baths, a kitchen, nurses quarters, hot and cold running water, and an ice water cooler. Windows circulated air through the wards, which held nearly 450 beds. During its four years of service, the DA January transported and cared for more than 23,000 wounded men. It regularly visited the cities along the Mississippi and Ohio rivers.